

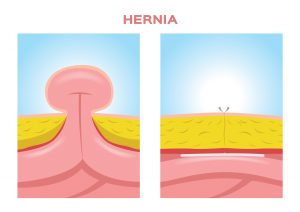
This is a little like a “blowout” in a bicycle tyre (where the inner tube is ‘squeezed’ out through a hole in the tyre). In the human body, the abdominal wall muscles (’the six pack’ so to speak) and the thick ‘belts’ of fibrous tissue between them serve to hold your ‘innards’ inside you. The ‘innards’ include bowel and fat (everyone has this inside them) which are the most relevant with respect to a hernia, however there are other structures inside as well. If the muscles have a ‘defect’ or a hole in them, then fat or bowel can push through as a ‘blowout’. This is the hernia itself and it would either be felt as a lump or a discomfort. It can be very small and subtle (causing no or minimal discomfort) to large and unsightly. Pressure rises inside the abdomen put pressure on the hernia to protrude so the natural history of a hernia is for it to increase in size. Pressure rises from abdominal wall muscle contraction can result from a number of things that include physical exercise, coughing or straining from constipation to pass stool.

FAQs
Why did I get a Hernia?
Either you were born with a tendency to have weak tissues at the site of the hernia, or you have developed a weakness such as from a previous surgery incision. Hernias are very common such that effectively if you develop one it is almost “one of those things” and the rest of your body otherwise and muscles can be very strong and robust (often athletes get hernias). In the groin on each side of the pubis everyone has a ‘weak spot’ for anatomical reasons – in men the blood vessels and a tube to the testicles need to pass through the muscles to the scrotum, and in females a ligament holding the uterus passes through it. At the umbilicus (belly button) is the site where the umbilical cord was connected to your mother and which needs to ‘close over’ after your birth so not to have a hernia from birth (it can still close over after birth but remain a weak spot for a hernia to occur later in life). During surgery the abdominal wall muscles are repaired with stitches and often mesh. The bulk of the healing at the incision occurs over a 6 week period. Other sites of hernia can also occur and potentially for both of these reasons.

Do I need surgery for my Hernia?
Historically hernias were repaired quite liberally when they presented in order to avoid the potential serious complication of bowel being caught passing through the hernia and developing gangrene. In modern practice, a clinical decision is made by your surgeon that accounts for all risks and benefits. Benefits of repairing the hernia include reducing the chance of a serious hernia related complication (like bowel strangulation), removing or reducing the pain from a hernia, ‘normalising’ the appearance of the abdomen by fixing an unsightly and awkward lump and improving quality of life and allowing a return to more normal activities. Note a small hernia can be as much of a problem and risk than a large one (a small hole in the muscles can still allow bowel to come through and the small hole can ‘strangle’ the bowel more easily than a large hole). Risks include any small risk from surgery or the chance of creating discomfort that may not be present in the first place for a small hernia. Assessing a person’s general fitness for surgery is also another important factor that your surgeon needs to consider in whether to operate or not.

What happens during Hernia surgery?
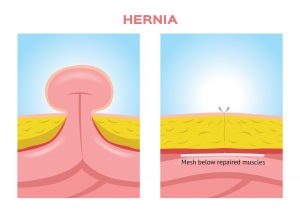
It is standard to have a general anaesthetic (although local anaesthetic can sometimes be an option). Laparoscopic or keyhole surgery is often preferred (due to less early post surgery pain and usually less scarring) although open surgery can provide better outcomes for you in certain circumstances and should be considered by your surgeon. The key elements of the surgery entail replacing the bowel or fat back inside the abdomen (sometimes excising excessive fat) and then repairing the hole. Usually the repair is done by strong permanent stitches and also mesh reinforcement. The mesh is used as the tissues around the hernia are often weak and why the hernia formed in the first place. The mesh provides a scaffold for your body to form strong scar tissue throughout it to keep the tissues solidly repaired and reduce the chance of the hernia coming back. In the case of an inguinal groin hernia in males it is necessary to leave a very small gap for the tube and blood vessel to the testicle. This is recreated through the mesh and the mesh provides strength at its edges. The skin is then stitched with dissolvable stitches and wound dressings applied. Local anaesthetic is inserted to ease any discomfort. Walking is encouraged as soon as possible after surgery.
Do I need mesh for my Hernia repair?
Not always but most hernia surgeons prefer to use mesh unless the hernia hole is very small and the surrounding tissues strong. The vast majority of surgeons use mesh for abdominal wall hernias and have done so for many decades. The mesh is made from sterile inert materials that include polyester and polyprolene and these are now both strong and soft (and it is placed quite deep to the skin so not to feel it). Many studies have proven that mesh significantly reduces the chance of the hernia coming back (and needing a second hernia operation is more problematic than the first). Using mesh on the abdominal wall is also quite a different scenario to using it next to an abdominal organ (such as mesh used by gynaecologists in surgery on female pelvic organs). When used on the abdominal wall the mesh is not in direct contact pressing on an organ, rather within the abdominal wall.
Should I only have keyhole/laparosacopic surgery for my hernia?
Laparoscopic or keyhole surgery is often preferred (due to less early post surgery pain, usually less scarring and less wound related issues) although open surgery can provide better outcomes for you in certain circumstances and should be considered by your surgeon. Every circumstance is different and indications are generally relative and not absolute. Groin hernias are well suited to keyhole surgery. For small to medium abdominal wall hernias from previous surgery, keyhole surgery is often a good option. Open surgery is often used for large abdominal hernias where the muscles need to be released to allow them to be stitched together. A skilled hernia surgeon should understand these issues and specifically assess your individual situation and discuss the risks and benefits of each.
What is the recovery after hernia surgery?
For inguinal, femoral, groin hernia surgery this is usually done as “day surgery” where you are admitted on the morning of surgery and discharged after surgery on the same day. You are walking within a few hours after surgery and you take pain killer tablets mostly in the first couple of days as your mobility increases. You should be walking freely after these few days and should be encouraged to do so. Gentle daily activities can be undertaken provided there is no significant discomfort. Light exercises could be undertaken after a couple of weeks. Exercises or work that involves significant pressure on the abdominal wall muscles should usually be avoided for around 6 weeks while the tissues heal, mesh incorporates and to reduce any discomfort. Work that involves desk work can usually be undertaken within the first week whilst more physical jobs or where significant driving/travel is involved a longer time period is needed.
What should I do now?
It is best to talk to your GP who will discuss with you about seeing an Upper Gastro-Intestinal Surgery specialist. You will need a referral from them to see Dr Le Page. You can choose a specialist of your choice in discussion with your GP. Dr Phil Le Page has performed around 1000 hernia operations and is specialised in this field and welcomes you to attend for a consultation.